Human Serum Albumin (HSA)
Identity
- Gene: ALB
- UniProt: P02768
- MW: ~66.5 kDa (native), 585 amino acids
- Plasma abundance: ~35–50 g/L (most abundant plasma protein, ~60% of total protein)
- Half-life: ~20 days
- Synthesis: exclusively by the liver (hepatocytes) → quantitative and qualitative changes directly reflect liver function
Biological function
HSA is the main carrier protein in blood. It transports fatty acids, hormones, drugs, metals (Cu²⁺, Zn²⁺), and bilirubin. It maintains oncotic pressure, buffering capacity, and antioxidant defense (via Cys34 free thiol). Because of its long half-life and high abundance, it acts as a recorder of systemic metabolic and oxidative stress — accumulated PTMs reflect the patient’s history over weeks.
Circulating isoform landscape
In plasma, HSA circulates as a mixture of up to 10 quantifiable isoforms in liver disease. In healthy subjects, the dominant forms are native and HSA+CYS:
| Isoform | PTM(s) | Δmass (Da) | Healthy % | Notes |
|---|---|---|---|---|
| Native HSA | None (Cys34 free) | 0 | ~20–30% | Fully reduced; antioxidant-competent |
| HSA+CYS | Cysteinylation Cys34 | +119 | ~70–80% | Most abundant normal form (human mercaptalbumin oxidized) |
| HSA+GLYC | Mono-glycation | +162 | low | Reflects glycemic exposure |
| HSA+CYS+GLYC | Cysteinylation + glycation | +281 | low | Combined modification |
| HSA+2GLYC | Double glycation | +324 | low | |
| HSA+CYS+2GLYC | Double glycation + cysteinylation | +443 | ~0 | End-stage marker — near-zero in healthy |
| HSA+SO₃H | Sulfonylation (irreversible) | +48 | low | Irreversible Cys34 oxidation |
| HSA-DA | N-terminal –Asp truncation | −115 | low | ⚠️ Higher in controls than in CLD patients |
| HSA-L | C-terminal truncation | variable | low | No change with CLD in ALBOM |
| HSA-DA+CYS | Truncation + cysteinylation | −115 +119 | low | ↓ in F4_B/C |
Known PTM sites
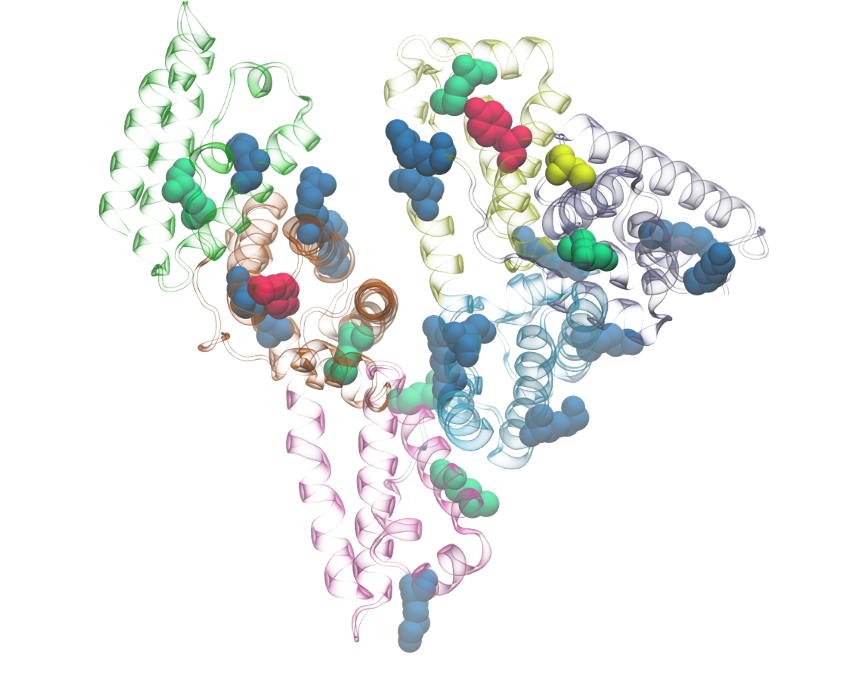
Potential post-translational modification sites mapped onto the albumin structure (molecular modelling, INSERM UMR1248 team).
| Residue | Position | Modification | Δmass (Da) | Biological role | Clinical relevance |
|---|---|---|---|---|---|
| Cys | Cys34 | Cysteinylation | +119 | Redox sensor — most reactive free thiol in plasma | Oxidative stress, liver disease, CLD staging |
| Cys | Cys34 | Glutathionylation | +305 | Redox | Oxidative stress |
| Cys | Cys34 | Sulfonylation (–SO₃H, irreversible) | +48 | Irreversible oxidation | Severe oxidative damage; ↓ in F4_B/C |
| Cys | Cys34 | Sulfinylation (–SO₂H, irreversible) | +32 | Oxidative damage | |
| Lys | Multiple (Lys4, Lys12, Lys51, Lys199, Lys525…) | Glycation (non-enzymatic) | +162 per site | Glucose adduct; multi-site | Diabetes, metabolic stress, CLD staging |
| Met | Multiple | Oxidation | +16 | Oxidative damage | Aging, inflammation |
| Trp | Trp214 | Oxidation | +4, +16, +32 | Damage to drug-binding site II | ⚠️ Limited clinical data |
| N-term | Asp1 | Truncation (−Asp) | −115 | N-terminal variant | ⚠️ Paradoxically ↓ in CLD vs controls |
| C-term | — | Truncation (–Leu or other) | variable | C-terminal variant | No significant change in CLD (ALBOM) |
Quantitative data from ALBOM study (el-balkhi-2025)
Native HSA concentrations across CLD stages:
| Stage | Native HSA (g/L) | AUC vs controls |
|---|---|---|
| Controls | 12.2 | — |
| F0/F1 | 10.6 | 0.67 |
| F2 | 9.9 | — |
| F3 | 10.6 | — |
| F4_A (Child-Pugh A) | 10.2 | — |
| F4_B (Child-Pugh B) | 4.1 | 0.99 |
| F4_C (Child-Pugh C) | 4.2 | 0.89 |
HSA+CYS peak: controls 8.7 g/L → F4_A 11.1 g/L (peak) → F4_B 7.9 → F4_C 6.8 g/L HSA+CYS+2GLYC: controls ~0 → F4_A 0.12 → F4_B 0.18 → F4_C 0.2 g/L (monotonically increasing)
Isoform patterns in chronic liver disease (3 types)
- Progressive decrease — truncation / irreversible oxidation: native HSA, HSA-DA, HSA+SO₃H, HSA-DA+CYS
- Biphasic — moderate oxidative/glycative stress: HSA+CYS, HSA+GLYC, HSA+CYS+GLYC, HSA+2GLYC
- Progressive increase — multiply-modified end-stage accumulation: HSA+CYS+2GLYC
The biphasic pattern creates an apparent paradox: the ratio (isoform/native HSA) correctly resolves it by normalizing for the overall fall in albumin synthesis — see hsa-isoforms-cld.
Analytical challenges
- Very high abundance masks low-abundance co-eluting proteins
- Extreme heterogeneity: hundreds of co-existing PTM combinations → complex mass spectrum
- Cys34 redox state changes ex vivo during sample handling (oxidizes rapidly) → requires careful pre-analytical control
- Top-down proteomics is the method of choice for intact isoform resolution
- Bottom-up proteomics loses PTM combinations and inter-site relationships
- High-mass glycated species (>67,500 Da, e.g. HSA+CYS+2GLYC) can be attenuated by baseline correction algorithms on some instruments (Bruker timsTOF Pro2 — actionable optimization target)
In our research
HSA is the central object of the ALBOM study and a primary target of the CQFD-PTM pipeline.
Key findings from el-balkhi-2025:
- 10 isoforms quantified across 172 CLD patients + 82 controls
- Three-class OrdinalForest classifier: QWK 0.862–0.916 vs FIB-4 QWK 0.188–0.229
- Cross-platform reproducibility confirmed (Bruker vs Sciex, McNemar p=0.149)
- HSA+GLYC/Native ratio: highest single-marker discrimination for F4_B (Sens 85%, Spec 100%)
- HSA+CYS+2GLYC: candidate end-stage marker (monotonically increases, near-zero in controls)
Key studies
el-balkhi-2025 — ALBOM publication (Scientific Reports 2026, DOI 10.1038/s41598-026-57614-y; Open Access)
HMA/HNA1/HNA2 nomenclature (Cys34 redox classification)
The IEC-based literature classifies HSA into 3 Cys34 redox fractions. These map onto the top-down isoform landscape:
| IEC fraction | Cys34 state | Δmass | TD isoform equivalent | Healthy fraction |
|---|---|---|---|---|
| HMA (mercaptalbumin) | Free thiol | 0 Da | Native HSA | 70–80% |
| HNA1 (nonmercaptalbumin-1) | Reversible oxidation (disulfide) | +119 Da | HSA+CYS | 20–30% |
| HNA2 (nonmercaptalbumin-2) | Irreversible oxidation (sulfinic/sulfonic acid) | +32/+48 Da | HSA+SO₃H (ALBOM: HSA+SULF) | ~5% |
- HNA2 >12% = poor 30/90-day prognosis in cirrhosis — oettl-2013
- HNA1 triggers cytokine storm in leukocytes via p38 MAPK — alcaraz-quiles-2018
- HNA2 hyperoxidation modulates neutrophils in severe AH — das-2017-sah
See Oxidation for the full Cys34 redox mechanism and mass spectral signatures.
Effective albumin (eAlb)
eAlb = tAlb (g/L) × native HSA fraction (%) / 100 — formally defined in baldassarre-2021-ealb.
- eAlb declines more steeply than tAlb across cirrhosis stages (compensated→AD→ACLF)
- eAlb at admission predicts 30-day ACLF and 90-day mortality better than tAlb
- eAlb connects quantity (tAlb by BCG) with quality (native fraction by LC-MS)
- See bernardi-2023 for the clinical paradigm perspective
HSA in acute liver failure (ALF)
In ALF (jaundice + encephalopathy within 4 weeks + INR >1.5, no prior CLD), albumin undergoes pronounced and rapid PTM accumulation proportional to mortality risk:
| PTM/marker | Non-survivors vs survivors | vs healthy |
|---|---|---|
| HNA2 (%) | ↑ (p=0.001) | ↑ (p=0.001) |
| AOS (HNA/HMA ratio) | ↑ (p=0.001) | ↑ |
| AGE, AOPP, IMA, IMAr | ↑ (p<0.001) | ↑ |
| HMA (%) | ↓ | ↓ |
| ABiC (albumin binding capacity) | ↓ (p<0.0001) | ↓ |
These changes mirror cirrhosis/ACLF but on an acute timescale (days–weeks). The Cys34 irreversible oxidation (HNA2) → functional impairment link is aetiology-independent (HEV vs DILI show identical patterns).
Beyond albumin structure, the albuminome (albumin-bound proteins, metabolites, lipids, and bacterial peptides) distinguishes non-survivors with near-perfect accuracy: AUC 0.98–0.999 across 4 omics arms. A 5-metabolite panel (nicotinic acid, L-acetyl carnitine, L-carnitine, pregnenolone sulfate, N-(3-hydroxybutanoyl)-L-homoserine lactone) validated at >92% accuracy and outperforms MELD (HR 5.81 by Cox regression). See sharma-2023 and acute-liver-failure.
Key studies
- el-balkhi-2025 — ALBOM publication; 10 isoforms; OrdinalForest classifier; cross-platform
- lakis-2024 — absolute quantification method (equine Mb IS); 8 isoforms
- rahali-2022 — TD vs BU validation; 15 isoforms by TD; 127-peptide BU library
- el-balkhi-2024-seb — SEB test; early detection in rat hepatotoxicity model (D3 vs D7 for ALT/AST)
- domenicali-2014 — seminal paper; 7 isoforms; native HSA predicts 1-year survival; foundational
- baldassarre-2016-dimers — HSA homodimers in cirrhosis; 3 dimer species; ACLF association
- baldassarre-2021-ealb — effective albumin; 11 isoforms; ACLF prediction; 90-day mortality
- oettl-2013 — HNA2 >12% predicts 30/90-day survival; IEC method
- naldi-2016-ah — HSA microheterogeneity in alcoholic hepatitis
- naldi-2017-review — comprehensive analytical review (all methods, all PTMs)
- alcaraz-quiles-2018 — HNA1 triggers cytokine storm via p38 MAPK
- das-2017-sah — hyperoxidized albumin modulates neutrophils in severe AH
- paar-2021 — SAXS: conformational opening in CLD HSA; cargo-driven (bilirubin/FA)
- spinella-2016-review — structure, functions, therapeutic implications in CLD
- montomoli-2026-aah — HSA isoforms in alcohol-associated hepatitis (n=49); no survival prediction at this n
- sharma-2023 — ALF albuminome; 200 ALF + 25 HC; HNA2↑/HMA↓ in NS; 5-metabolite panel AUC 0.98; outperforms MELD
Open questions
- What is the etiology-specific isoform fingerprint (MASH vs. ALD vs. viral)?
- Can longitudinal tracking of HSA isoform ratios predict clinical decompensation or response to therapy?
- Is there a minimal panel of isoform ratios deployable as LC-MRM-MS or immunoassay for broader clinical use?
- What drives the HSA-DA paradox (higher in controls than CLD at all stages)?
- How stable are HSA PTMs under different sample storage conditions?
- Can the HSA+DHA (dehydroalanine) isoform be reliably detected and quantified in clinical samples?
- Does homodimerization (hdHA-DA, hdHA-L, hdHA-native) contribute significantly to the effective albumin deficit in ACLF patients?